N-of-1: The Scorned Sleeping Beauty of Mainstream Medicine
Last updated: Oct 01, 2024
“Reduce your salt intake to lower your blood pressure.” You have probably heard that message. What you may not have heard is that it may be bad advice for one of six readers. If you are one of those, skimping on sodium may drive your blood pressure up not down.
This real phenomenon of the inverse salt-sensitive person doesn’t fit into mainstream medicine’s one-size-fits-all paradigm. Its claim to being evidence-based comes from group-based trials that look at averages of effects over groups of trial participants. But as every statistician knows, translating group-based evidence to an individual is a fallacy.
Group averages conceal the fact that the average participant does not fully represent most participants (if they exist at all). Neither does the average patient. This brings me to the heart of N-of-1: It turns the individual into a clinical trial, that aims at uncovering the only evidence that counts for that individual: his or her individual response to the intervention in question.
Nowhere is that more important than in the context of preventive lifestyle medicine.
OK, I admit I’m biased. You can probably think of many other equally important fields that may not even reside within medicine. But those are not the topics of this post. This post is all about my admittedly blinkered view of N-of-1 as the potentially most momentous, yet largely ignored tool for the medicine of successful aging.
We have reached a unique opportunity in medicine. For about the past 15 years, we have been able to predict health and life expectancy for any given individual much more accurately than ever before.
The discovery of aging-associated patterns of epigenetic change — cytosine methylation — across the life span gave rise to the idea of biological clocks that estimate a person’s biological age as distinct from their calendar age (Bocklandt et al, 2011). Of the epigenetic clocks, the Horvath clock is one of the best investigated (Guevara and Lawler, 2018). The logical next step was to correlate these patterns with health and survival outcome.
What these clocks all have in common is that accelerated and decelerated biological aging correlate with shorter or extended health span and lifespan respectively. The clocks’ main drawbacks are that (a) we don’t know yet how their epigenetic patterns causally relate to the chronic diseases of aging, and (b) different clocks come to different conclusions, sometimes even for different organs within the same individual (Bergsma and Rogaeva, 2020). They are also impractical in the context of N-of-1 single-case experiments as they require access to special labs and costly analytics.
Now imagine: What if we could find a modifiable and causative metric of biological age, make it accessible to laypersons, and operationalize N-of-1 methods as a lay-capable DIY tool to estimate and optimize lifestyle interventions’ effects on health span and lifespan?
No more flying blind with respect to how any recommendation, like sodium reduction, will affect one’s own health and life expectancy (rather than on average). After all, life doesn’t come with a reset button, which you hit at age 70 after realizing that your chosen health habits didn’t deliver the hoped-for dividends.
That’s what my team and I have set out to achieve.
Our research and clinical focus on cardiovascular medicine made the choice of biomarker an obvious one: vascular function.
We have known for 300 years that “Man is as old as his arteries” (attributed to Thomas Sydenham). When it comes to vascular aging, there are three scenarios: The unfavorable one, called “early vascular aging” (EVA), the favorable one, called “super-normal vascular aging” (SUPERNOVA), and the one in-between, called “normal” vascular aging (Bruno et al, 2020).
In all three, pulse wave velocity (PWV) plays the lead role. PWV is the speed at which the blood pressure wave travels through the arterial tree, ranging from below 5 to more than 20 m/s (Baier et al, 2018).
PWV is determined by the vessel’s elasticity or compliance. As a rule of thumb, the healthier (biologically younger) the vessels, the more compliant they are, and the slower the PWV. I have explained the relevance of PWV in another blog post on Medium.
Our first step was to translate PWV into a biomarker for vascular age. From our research pool of subjects, ranging across all ages and health conditions, we were able to extract an algorithm that expresses vascular age in relation to chronological age (Kraushaar et al, 2017).
In follow-up research, we included a special cohort of successful agers (medication-naïve individuals >65 years without any chronic conditions). This enabled us to derive a metric for the rate of aging in relation to chronological aging.
For a long time, the measurement of PWV was confined to doctor’s practices and special labs like ours. However, the company Withings developed a bathroom scale that applies ballistocardiography (“a measure of ballistic forces generated by the heart”) to determine PWV. The validity of their method and devices has been independently validated (Campo et al, 2017).
Our second step was to recalibrate our algorithm to the “Withings PWV”, which measures PWV over a slightly different path (from heart to foot) than our original measure, brachial-ankle PWV (baPWV). We used consecutive baPWV and Withings PWV measurements taken from a convenience sample of subjects as the basis for our algorithm. While small in absolute numbers, the sample contained female and male participants of various heights (from 150 cm to 192 cm).
Our third step was to create a web application that operationalizes the N-of-1 approach for investigating what affects one’s own PWV. Laypersons would be able to use our web application to design and implement their own N-of-1 trial, with PWV as the main outcome or “primary endpoint” for assessing the effectiveness of their trial-and-error lifestyle medicine interventions.
Currently, our web application runs on our medical-grade server on top of telemedicine architecture provided by Monitored Therapeutics. Their architecture has been used for many years by several prominent clinics in the US (e.g., Mayo Clinic, Cleveland Clinic, MD Anderson, Johns Hopkins Medicine, UNC School of Medicine).
A key feature and purpose of the telemedicine architecture is the remote monitoring of biomarkers such as blood pressure, blood sugar, heart rate, and others). Measurement devices that are capable of communicating their data via WLAN to our server enable users/patients and their health coaches/doctors to monitor the relevant biomarker(s) in real-time, and to alert coaches/doctors to any untoward developments or trends.
We have now integrated the Withings scale into this architecture, whereby our server polls via API the Withings server for the relevant measurement data.
To keep it simple and accessible, we currently enable AB designs only. The reason: in lifestyle medicine, alternating intervention phases (B-phases) with baseline phases (A-phases) in which the intervention is suspended is often not feasible or ethical. A smoker whose intervention is the cessation of smoking will hardly want to go back to baseline just for experimental reasons.
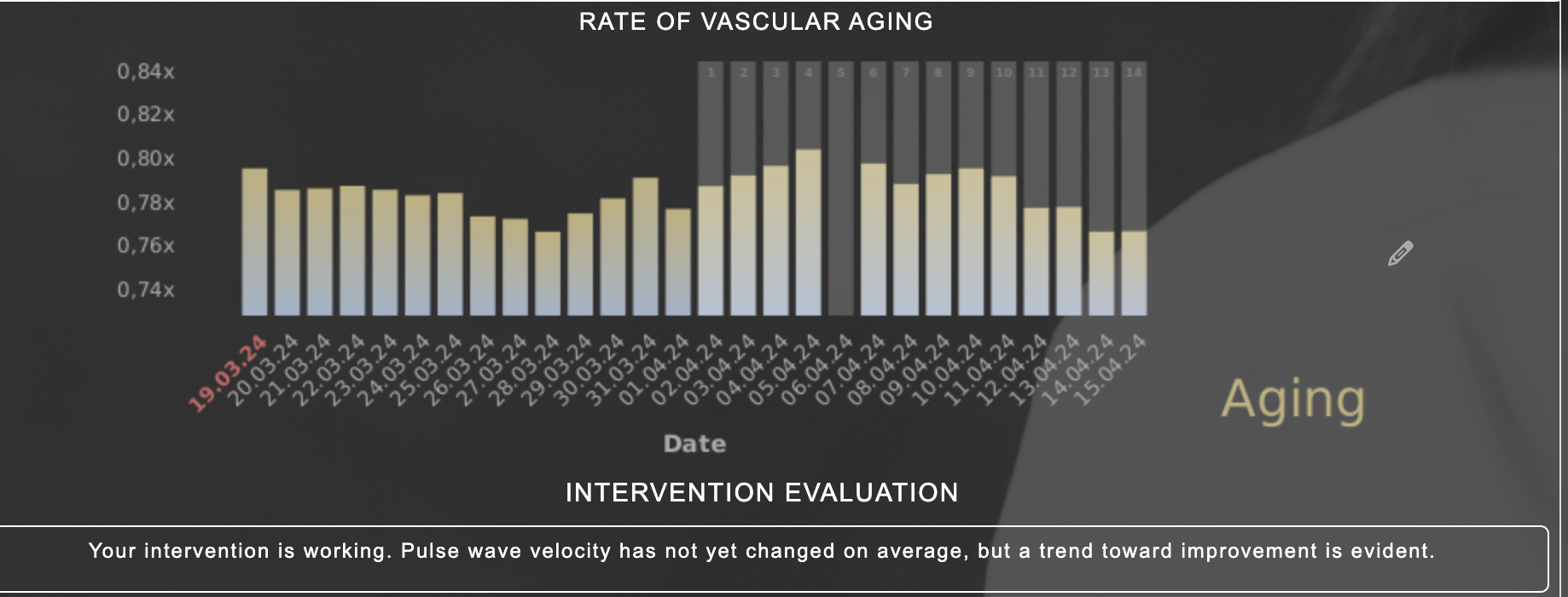
Our current system allows the participant to investigate intervention outcomes like phase differences, trends within phases, and differences of trends. The system allows them to define a measure of their own average effects, and provides daily feedback on results in a graphical and intuitively understandable way.
We are aware that our current system only scratches the surface of what this powerful method of single-case research has to offer. It will certainly not be the final iteration. We currently collect feedback on practical issues and user acceptance from beta-testers worldwide.
I still do not comprehend why mainstream medicine hasn’t adopted N-of-1 into its arsenal of individualized medicine.
The decoding of the human genome raised exaggerated expectations about the ability to predict not only disease risk but also the effects of interventions from reading the blueprint of the human organism (Schork, 2015; Senn, 2018). Today, we know that the hundreds of gene polymorphisms that correlate with chronic diseases have only weak predictive power. We also know that the latter is confounded not only by interactions between genes, but also with environment, behavior, microbiome, and epigenetics. We are nowhere near the ideal of forecasting health from readings of the genomic blueprint.
We also know that our one-size-fits-all recommendations and interventions fail many individuals. They mistakenly assume that population-average effects apply well to individuals. This renders them clinically inaccurate for each patient, if not irrelevant or even detrimental.
The one takeaway of our approach and web tool that has impressed me most is the degree of interindividual variability of health profiles, preferred interventions, and biomarker responses. No two of our beta testers share the same profile, health objectives, or responses. This is ample evidence for the fallacy of one-size-fits-all recommendations embodied in the salt reduction paradigm.
In the context of preventive lifestyle medicine, N-of-1 methods offer a way out of the ineffectiveness that is the hallmark of today’s preventive medicine. This is why I have great hopes for approaches like ours to reform lifestyle medicine, one person at a time.
- Baier D, Teren A, Wirkner K, Loeffler M, Scholz M. Parameters of pulse wave velocity: determinants and reference values assessed in the population-based study LIFE-Adult. Clin Res Cardiol 2018. doi:10.1007/s00392-018-1278-3.
- Bergsma T, Rogaeva E. DNA Methylation Clocks and Their Predictive Capacity for Aging Phenotypes and Healthspan. Neurosci Insights 2020;15. doi:10.1177/2633105520942221.
- Bocklandt S, Lin W, Sehl ME, Sánchez FJ, Sinsheimer JS, Horvath S, et al. Epigenetic Predictor of Age. PLoS One 2011;6:e14821.
- Bruno RM, Nilsson PM, Engström G, Wadström BN, Empana JP, Boutouyrie P, et al. Early and supernormal vascular aging: Clinical characteristics and association with incident cardiovascular events. Hypertension 2020:1616–24. doi:10.1161/HYPERTENSIONAHA.120.14971.
- Campo D, Khettab H, Yu R, Genain N, Edouard P, Buard N, et al. Measurement of Aortic Pulse Wave Velocity With a Connected Bathroom Scale. Am J Hypertens 2017;30:876–83. doi:10.1093/AJH/HPX059.
- Guevara EE, Lawler RR. Epigenetic Clocks. Evol Anthropol 2018;27:256–60. doi:10.1002/evan.21745.
- Kraushaar LE, Christmann J, Sonntag A, Schmidt N, Dressel A, Kleber ME, et al. It is vascular age that matters: How arterial functionomics enhances biomarker based diagnostics. Biomarkers Cardio-Renal Axis, Mannheim, Germany: D-A-CH Association for Prevention of Cardiovascular Disease; 2017. doi:10.13140/RG.2.2.12654.41283.
- Schork NJ. Personalized medicine: time for one-person trials. Nature. 2015 Apr 30;520(7549):609-11. doi:10.1038/520609a.
- Senn S. Statistical pitfalls of personalized medicine. Nature. 2018 Nov 27;563:619-621. doi:/10.1038/d41586-018-07535-2.
Lutz E. Kraushaar is a longevity researcher on a mission to rewrite the aging playbook using N-of-1 methods. His qualifications to do so include a doctorate in Public Health Sciences from Bielefeld University, Germany and a MSc. in Exrx & Nutrition from Chester University, UK. Lutz has focused his research work on the individualization of lifestyle medicine with the objective to expand people’s health span and lifespan. To that end he developed a biological clock based on arterial function as the primary biomarker. Together with his team he has operationalized N-of-1 methods into a web application accessible to laypersons.